 Endometriosis is the most mysterious gynecological disorders. It is the occurrence of ectopic endometrial tissues outside the cavity of the uterus. These islands of endometriosis are composed of endometrial glands surrounded by endometrial stroma, which are capable of responding to a varying degree to cyclical hormonal stimulation.1
Endometriosis is the most mysterious gynecological disorders. It is the occurrence of ectopic endometrial tissues outside the cavity of the uterus. These islands of endometriosis are composed of endometrial glands surrounded by endometrial stroma, which are capable of responding to a varying degree to cyclical hormonal stimulation.1
Aetiology
Endometriosis is a disease of the child- bearing period. Its incidence appears to be on the increase, partly due to improvement in diagnostic techniques and partly due to changing social patterns like late marriage and limitation of family size. It has been seen that it tends to occur more amongst the affluent class, and is frequently associated with infertility.1
Below are some theories to explain endometriosis1
- Implantation theory
- Coelomic metaplasia theory
- Metastatic theory
- Histogenesis by induction
- Hormonal influence
- Immunological factor
- Other factors – genetic, vaginal or cervical atresia
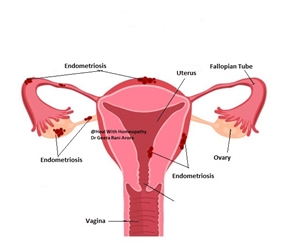
Sites1
- Ovaries
- Cul-de-sac
- Uterosacral ligaments
- Peritoneum overlying the bladder
- Sigmoid colon
- Back of the uterus
- Intestinal coils
- Appendix
- Lower pelvis
- Umbilicus
Pathology
An endometriotic area appears as a dark red, bluish or black cystic area, adherent to the site where it is lodged. Scarring around the endometriosis gives a puckered look. Lately, atypical lesions such as no pigmented areas or yellowish whit thick plaques have been noticed. Peritoneal cavity contains yellowish brown fluid in the cul-de-sac and this contains prostaglandin responsible for pain.1
Chocolate cysts of the ovaries represent the most important manifestation of endometriosis. To the naked eye, the chocolate cyst shows obvious thickening of tunica albuginea, and vascular red adhesions are well marked on the under surface of the ovary. The inner surface of the cyst wall is vascular and contains areas of dark brown tissue.1
There are three categories of endometriosis and each has a different mode of development1
- Pelvic endometriosis may be localized or diffused and scattered over the pelvic peritoneum, pouch of Douglas and utero-sacral ligaments.
- Ovarian endometriosis or chocolate cyst.
- Rectovaginal endometriosis.
Classification1
The Classification is correlated with fertility outcome rather than pain symptom
- Minimal: Small spots of endometriosis seen at laparoscopy, but no clinical symptoms.
- Mild: Scattered fresh superficial lesions. No scarring or retraction. No adnexal adhesions.
- Moderate: Ovaries are involved, with some scarring and retraction. They contain endometriomas not more than 2 cm in size. There are minimal peritubal and periovarian adhesions. Endometriotic lesions in the anterior and posterior peritoneal pouch with some scarring and retraction may be seen.
- Severe: Ovaries are involved, with the size of the endometriomas exceeding 2 cm. dense peritubal and per ovarian adhesions severely restrict mobility. The uterosacral ligaments are thickened and involved and lastly, there may be evidence of involvement of the bowel and urinary tract.
- Laparoscopic findings vary with the duration of the lesion, size and location. ‘Powder-burn’—puckered black spots, red vascular, bluish, blackish cysts, chocolate cysts and dense adhesions in the pelvis as well as yellow-brown peritoneal fluid are the findings.
Poor correlation between the naked eye appearance and histology is well documented. Therefore, biopsy of the suspicious areas becomes necessary to prove the presence of endometriosis.1
Clinical Features
Endometriosis affects women in the reproductive age, around 30 years. It may occur in an adolescent if obstruction in the lower genital tract causes cryptomenorrhoea and retrograde spill of menstrual fluid. A rare case of endometriosis has been reported in a postmenopausal woman on hormone replacement therapy (HRT).1
Symptoms
 The symptoms vary according to the site, depth of lesion and do not always correlate well with the extent of disease. The classic symptom complex includes dysmenorrhoea, dyspareunia, menorrhagia and infertility. About 30% of the patients are asymptomatic. Overlapping of symptoms is common.1
The symptoms vary according to the site, depth of lesion and do not always correlate well with the extent of disease. The classic symptom complex includes dysmenorrhoea, dyspareunia, menorrhagia and infertility. About 30% of the patients are asymptomatic. Overlapping of symptoms is common.1
The following are the common symptoms1
- Dysmenorrhoea
- Abdominal pain
- Dyspareunia
- Infertility
- Menstrual symptoms
- Chronic pelvic pain (CPP)
Differential Diagnosis1
- Chronic pelvic inflammatory disease closely mimics endometriosis in its symptoms and signs. Both the conditions produce pelvic pain, congestive dysmenorrhoea, menorrhagia and sterility.
Endometriosis may, if there is leakage of blood contents, produce leucocytosis, raised ESR and moderate fever. Also, both have similar physical signs. Laparoscopic visualization of the pelvis will reveal the true pathology.
- Uterine myomas, unless degenerate, are painless and the uterus is not fixed. Ultrasound and laparoscopic visualization will differentiate on condition from the other.
- Ovarian malignant tumor with metastatic deposits in the pouch Douglas can be mistaken for endometriosis.
- Recto sigmoid involvement will cause rectal symptoms which resemble the symptoms of rectal carcinoma. It may be impossible to make an accurate diagnosis until sigmoidoscopy and biopsy are performed.
- If the chocolate cyst ruptures, all possibilities of an acute abdominal catastrophe must be considered, including a ruptured tubal gestation, though the most frequent error is to operate for acute appendicitis.
- Chronic pelvic congestion syndromes due to other causes must be excluded by ultrasound, CT, MRI and laparoscopy.
Investigations1
- Laparoscopic Findings
-
- To detect and diagnose pelvic endometriosis.
- Locate the site of endometriosis and staging.
- To take biopsy.
- Ultrasound and MRI
- Prophylaxis
Management
Minimal asymptomatic cases should be observed over 6–8 months. Infertility should be investigated and treated as necessary.1
All symptomatic women need treatment. The treatment depends upon the age of the patient, need forpreserving reproductive functions, severity of the symptoms, extent of the disease, response to medical treatment, relief obtained with any previous conservative surgery andthe attitude of the patient towards her problem. The objective of the treatment should be to eradicate the lesion andavoid recurrence of the disease process, alleviate symptoms, facilitate childbearing and enable the patient to leada comfortable life. Therefore, the treatment should be individualized. The treatment comprises medical surgical and a combination of both.1
There are many medicines in homeopathic literature which indicates its usage for endometriosis. A well selected homeopathic remedy and one based on pathological action of remedy can help treat this condition. Many acute medicines are available to help in pain relieving due to endometriosis which shall be supplemented by a deep acting remedy which will correct the condition. The treatment shall be individual based treatment.
Few Medicines for Endometriosis
 Lachesis mutus
Lachesis mutus
Nymphomania; uterine region feels swollen, will bear no contact; bearing-down pains; uterine and ovarian pains relieved by a flow of blood; pains like knife thrust into abdomen; uterus feels as if os were open; redness and swelling of external parts, with discharge of mucus; swelling, induration, neuralgia, suppuration, etc., of left ovary; pain in coccyx when sitting down, as if sitting on something sharp; trembling of legs; cervix very sensitive to touch, bleeding easily.
 Lilium tigrinum
Lilium tigrinum
Uterine symptoms following pregnancy and labor; subinvolution, uterus does not regain its normal size after confinement, when rising to walk, uterus falls by its own weight; heavy dragging sensation, principally in hypogastric region; she feels the need of some support to hold the abdominal organs up, sensation of dragging down from shoulders and chest.
Active congestion, with great nervous irritability and local pain and sensitiveness; prolapse or anteversion; bladder affected.
 Lycopodium clavatum
Lycopodium clavatum
Swelling of ovaries and of uterus; cutting across the hypogastrium from left to right; ovaries diseased, ovarian tumors, weariness, extreme weakness, emaciation, with tremors of limbs; stiffness, aching, chilliness, in small of back;
 Sabina
Sabina
Soreness of abdominal muscles; pressing down towards genitals; frequent and violent urging to urinate, with profuse discharge; hemorrhages, pale-red and clotted, or of very thin, discolored, offensive-smelling blood; foetidleucorrhoea after suppressed menses; condylomata, with sore, burning pains; better in open air;
Active congestion, with tendency to florid hemorrhage, accompanied by irritation of bladder and bowels
 Sepia officinalis
Sepia officinalis
Prolapsus uteri from atonic relaxation of the ligaments that supports of uterus, relieved by lying down or crossing legs; worse when sitting up, standing or walking, which causes bearing down, heat, soreness, backache and fainting; gone sensation in pit of stomach, about noon, relieved by eating and lying down; induration of neck of uterus; dropsy of uterus.
 Caulophyllum thalictroides
Caulophyllum thalictroides
Weak, delicate women; anteversion with flexion and uterine contraction; prolapsus and leucorrhoea the effects of atony, with weakness of legs and spasmodic, crampy, fitful or sharp pains here and there; leucorrhoea of profuse mucus; pains continue a long time after the attempt; constant desire to remain quiet.
 Cimicifuga racemosa
Cimicifuga racemosa
Irritable weakness; overwhelming apprehensiveness; prolapsus from deficient innervation and muscular atony with pain in hypogastric region; retroversion; great tenderness of uterus to pressure; spasms of broad ligaments; sharp pains across hypogastrium, aggr. from standing and motion; bearing down in uterine region and small of back, with tightness around hips; menses scanty, retarded or suppressed from different causes; subinvolution after miscarriage.
 Murex purpurea
Murex purpurea
Prolapsus with uterine pains extending upward from right side of uterus, crossing the body to the left mamma (Lil., from chest to uterus); pain in uterus as if cut by a sharp instrument; uterus feels dry, as if constricted; myalgic pain in uterus, coming on when in bed, amel. by sitting or walking, until tired out, when she must lie down for temporary relief, as the cutting pains come on again, going through her up diagonally, compelling her to get up again and walk.
 Platinum metallicum
Platinum metallicum
Induration of uterus; ulceration, with coexisting ovarian irritation; nymphomania, tingling or titillation from genitals up into abdomen; metrorrhagia, with great excitability of sexual system; pruritus vulvae, with anxiety and palpitation of heart; prolapsus uteri, with continual pressure in genital organs; numbness and coldness of body; melancholy; great sensitiveness of genitals, it hurts her to sit down; neuralgia uteri
 Pulsatilla pratensis
Pulsatilla pratensis
Prolapsus uteri, worse on lying down and from heat, better in fresh air, with pressure in abdomen and small of back as from a stone; limbs tend to go to sleep; ineffectual urging to stool; suppressed menses, pains in back and chilliness; crampy constriction in vagina; peevishness, with weeping; dimness of vision; pressure on bladder, frequent and copious micturition, without any strangury.
 Secale cornutum
Secale cornutum
Uterine ulcer, feels as if burnt, discharges putrid, bloody fluid; burning pains in the greatly distended uterus, which feels hard and is painful to the touch; ulcers on outer genitals discolored and rapidly swelling; brownish and offensive leucorrhoea; atonic, passive hemorrhage of very foetid or dark blood, worse from slightest motion; cold extremities, cold sweat, great weakness, small pulse, aggr. from warmth, motion, touching the parts. Subinvolution of uterusand displacements following parturition.
 Staphysagria
Staphysagria
Prolapsus uteri with flabby condition of stomach and abdomen, which feel as if they would drop out from relaxation; granular vegetations of vagina, leucorrhoea yellow and excoriating; stinging itching in vulva; nervous weakness
 Tarentula hispanica
Tarentula hispanica
Neuralgia of uterus, with sadness and despair, reflex chorea; hyperaemia and hyperaesthesia of sexual organs; fibrous tumors of uterus, with bearing-down pains; displacements of uterus, with retention of urine and difficult defaecation; sensation of great weight, with burning in hypogastrium and uterus.
 Arnica Montana
Arnica Montana
Prolapsus uteri, caused by a concussion, leaving a sore, bruised feeling in uterine region, preventing her from walking erect; metrorrhagia after coition; bloody discharge between the menstrual periods; ulcers of uterus with a tendency to bleed; riding on a rough road causes a flow of bright-red blood.
 Conium maculatum
Conium maculatum
Induration and enlargement of ovary, with lancinating pains; stinging in neck of uterus; induration and prolapsus at the same time; chronic pressive inflammation of ovaries; pressure and cutting pains in uterus when urinating; weight and lancinating pains in ovaries and uterus; extending through lower part of abdomen, hips and back; burning, stinging, darting pains in neck of womb, with scirrhous indurations.
 Palladium metallicum
Palladium metallicum
Symptoms of falling of womb with weeping mood, all motions are painful, she can hardly stand or walk; right side of abdomen (ovary) swollen, hard and painful as if beaten, with shooting pains from navel to pelvis, all on right side; heaviness as from a load with pressure deep in the pelvis, amel. When lying on left side; weakness as if the womb was sinking; empty feeling in groins as if eviscerated;
 Foods that may negatively affect endometriosis
Foods that may negatively affect endometriosis
- Alcohol
- Caffeine
- Gluten
- Red meat
- Saturated and trans fat
Foods that may positively affect Endometriosis
- Fibrous foods - fruits, vegetables, legumes, and whole grains.
- Iron-rich foods - dark leafy greens, broccoli, beans, fortified grains, nuts, and seeds.
- Foods rich in fatty acids - such as salmon, sardines, herring, trout, walnuts, chia, and flax seeds.
- Antioxidant-rich foods - colorful fruits and vegetables - such as oranges, berries, dark chocolate, spinach, and beets.
References
- Howkins &Bourne Shaw’s Textbook of Gynaecology. 16threv.ed. New Delhi: B.I. Churchill Livingstone; 1999. 584p.
- Dewey WA.Practical homeopathic therapeutics.3rd ed.New Delhi: B. Jain Publishers(P) LTD.;2009.
- Clarke JH.The prescriber.6th ed.New Delhi:B. Jain Publishers(P) LTD.;2011.
- Lilienthal, S. Homoeopathic therapeutics. Philadelphia: Boericke& Tafel; 1907