 Diabetes mellitus is a clinical syndrome characterized by anincrease in plasma blood glucose (hyperglycemia). It has many causes, most commonly type 1 or type 2 diabetes.1
Diabetes mellitus is a clinical syndrome characterized by anincrease in plasma blood glucose (hyperglycemia). It has many causes, most commonly type 1 or type 2 diabetes.1
Type 1 diabetes is generally considered to result from autoimmunedestruction of insulin-producing cells (β cells) in the pancreas,leading to marked insulin deficiency, whereas type 2 diabetesis characterized by reduced sensitivity to the action of insulinand an inability to produce sufficient insulin to overcome this‘insulin resistance’. Hyperglycemia causes both acute andlong-term problems. Acutely, high glucose and lack of insulincan result in marked symptoms, metabolic decompositionand hospitalization. Chronic hyperglycemia is responsible fordiabetes-specific ‘micro vascular’ complications affecting theeyes (retinopathy), kidneys (nephropathy) and feet (neuropathy).There is a continuous distribution of blood glucose in thepopulation, with no clear division between people with normalvalues and those with abnormal ones.1
DIAGNOSIS1
 The diagnostic criteria fordiabetes (a fasting plasma glucose of ≥ 7.0 mmol/L (126 mg/dL) or glucose 2 hours after an oral glucose challenge of≥ 11.1 mmol/L (200 mg/dL); p. 726) have been selected toidentify a degree of hyperglycemia that, if untreated, carries asignificant risk of micro vascular disease, and in particular diabeticretinopathy. Less severe hyperglycemia is called ‘impairedglucose tolerance’. This is not associated with a substantial riskof micro vascular disease,but is connected with an increasedrisk of large-vessel disease (e.g. atheroma leading to myocardial infarction) and with a greater risk of developing diabetesin future.1
The diagnostic criteria fordiabetes (a fasting plasma glucose of ≥ 7.0 mmol/L (126 mg/dL) or glucose 2 hours after an oral glucose challenge of≥ 11.1 mmol/L (200 mg/dL); p. 726) have been selected toidentify a degree of hyperglycemia that, if untreated, carries asignificant risk of micro vascular disease, and in particular diabeticretinopathy. Less severe hyperglycemia is called ‘impairedglucose tolerance’. This is not associated with a substantial riskof micro vascular disease,but is connected with an increasedrisk of large-vessel disease (e.g. atheroma leading to myocardial infarction) and with a greater risk of developing diabetesin future.1
The incidence of diabetes is rising. Globally, it is estimatedthat 415 million people had diabetes in 2015 (10% of theworld adult population), and this figure is expected to reach642 million by 2040. This global pandemic principally involves type 2 diabetes;prevalence varies considerably around the world, being associated with differences in genetic factors,as well as environmental ones such as greater longevity, obesity,unsatisfactory diet, sedentary lifestyle, increasing urbanization andeconomic development. A pronounced rise in the prevalence oftype 2 diabetes occurs in migrant populations to industrialized countries, as in Asian and Afro-Caribbean immigrants to the UKor USA. Type 2 diabetes is now seen in children and adolescents,particularly in some ethnic groups such as Hispanics, non-Hispanicblacks and Asian Indians.1
CLINICAL FEATURES2
- Common presenting symptoms of DM include polyuria, polydipsia, weight loss,fatigue, weakness, blurred vision, frequent superficial infections, and poor woundhealing. In early type 2 DM, symptoms may be more subtle and consist of fatigue,poor wound healing, and paresthesias.2
- The lack of symptoms is the main reason forthe delayed diagnosis of type 2 DM. Many patients are diagnosed based on screening orduring blood tests taken for other reasons. A complete medical history should beobtained with special emphasis on weight, exercise, smoking, alcohol consumption, family historyof DM, and risk factors for cardiovascular disease. In a patient with established DM,assessment of prior diabetes care, HbA1c levels, self-monitoring blood glucose results,frequency of hypoglycemia, and patient’s knowledge about DM shall be obtained.2
- Specialattention should be given on physical examination to retinal examination, BP,foot examination (including vibratory sensation and monofilament testing), peripheralpulses, and insulin injection sites. Acute complications of DM that may be seenon presentation include diabetic ketoacidosis (DKA) (type 1 DM) and hyperglycemic hyperosmolar state (type 2 DM).2
Glycated hemoglobin:
Glycated hemoglobin provides an accurate and objective measure of glycaemic control over a period of weeks tomonths.In diabetes, the slow non-enzymatic covalent attachment ofglucose to haemoglobin (glycation) increases the amount in theHbA1 (HbA1c) fraction relative to non-glycated adult hemoglobin(HbA0). These fractions can be separated by chromatography.1
Urine protein
Standard urine dipstick testing for albumin detects urinaryalbumin at concentrations above 300 mg/L, but smaller amounts(microalbuminuria; can only be measuredusing specific albumin dipsticks or quantitative biochemicallaboratory tests. Microalbuminuria or proteinuria, in the absenceof urinary tract infection, is an important indicator of diabeticnephropathy and/or increased risk of macro vascular disease.1
When a diagnosis of diabetes is confirmed, other investigationsshould include plasma urea, creatinine and electrolytes, lipids,liver and thyroid function tests, blood or urine ketones, andurine protein.1
AETIOLOGY AND PATHOGENESIS OFDIABETESF diabetes
- In both of the common types of diabetes, environmental factorsinteract with genetic susceptibility to determine which peopledevelop the clinical syndrome, and the timing of its onset.However, the underlying genes, precipitating environmentalfactors and path physiology differ substantially between type1 and type 2 diabetes.1
- Type 1 diabetes was previously termed‘insulin-dependent diabetes mellitus’ (IDDM) and is invariablyassociated with insulin deficiency requiring replacement therapy.1
- Type 2 diabetes was previously termed ‘non-insulin-dependentdiabetes mellitus’ (NIDDM) because patients retain the capacity tosecrete insulin, and measured insulin levels are often higher thanthose seen in people without diabetes. In type 2 diabetes, though,there is an impaired sensitivity to insulin (insulin resistance) and,initially, affected individuals can usually be treated without insulinreplacement therapy. However, 20% or more of patients with type 2 diabetes will ultimately develop insulin deficiency requiringreplacement therapy, so IDDM and NIDDM were misnomers.1
PROBLEMS IN DIABETES MELLITUS1
Hyperglycaemia
Symptoms:
- Thirst, dry mouth
- Polyuria
- Nocturia
- Tiredness, fatigue, lethargy
- Change in weight (usuallyweight loss)
- Blurring of vision
- Pruritus vulvae, balanitis(genital candidiasis)
- Nausea
- Headache
- Hyperphagia; predilection forsweet foods
- Mood change, irritability,difficulty in concentrating,apathy
The aims are to improve symptoms of hyperglycemia andminimize the risks of long-term micro vascular and macro vascularcomplications. Treatment methods for diabetes include dietary/lifestyle modification, oral ant diabetic drugs and injected therapies. In patients with suspected type 1 diabetes, urgent treatment withinsulin is required and prompt referral to a specialist is usuallyneeded. In patients with suspected type 2 diabetes, the firstapproach to management involves advice about dietary andlifestyle modification. Oral ant diabetic drugs are usually addedin those who do not achieve glycaemic targets, or who havesymptomatic hyperglycemia at diagnosis and a high HbA1c.However, the guidelines in some countries are to introducemedication immediately on diagnosis of diabetes without waitingto assess the impact of diet and lifestyle changes. Patientswith type 2 diabetes who present with marked symptomatichyperglycemia or DKA will require initial management withinsulin treatment.1
For most people, types 1 and 2 diabetes are chronic conditionsthat will impact on their day-to-day activities and require sustainedchanges to lifestyle. Education is key to achieving and maintaininga healthy lifestyle and to managing diabetes. Early educationalintervention at diagnosis and repeated education are essentialif these goals are to be successfully achieved. Management ofpeople with diabetes should be individualized where possible,taking into account personal and cultural beliefs, individualcircumstances, co morbidities and other factors.1
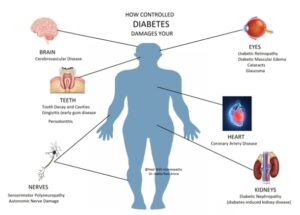
COMPLICATIONS OF DIABETES1
MICRO VASCULAR/NEUROPATHIC:
Retinopathy, cataract
- Impaired vision
Nephropathy
- Renal failure
Peripheral neuropathy
- Sensory loss
- Pain
- Motor weakness
Autonomic neuropathy
- Gastrointestinal problems(gastro paresis; altered bowelhabit)
- Postural hypotension
Foot disease
- Ulceration
- Arthropathy
MACRO VASCULAR:
Coronary circulation
- Myocardial ischaemia/infarction
Cerebral circulation
- Transient ischaemic attack
- Stroke
Peripheral circulation
- Claudication
- Ischaemia
SCOPE OF HOMEOPATHY: Diabetes is a lifestyle condition and Homeopathy can help in various ways. There are some medicines which help is control blood glucose levels which are available over the counter. These can be helpful in cases where patient is managing with lifestyle change and has rise of blood sugar to a mild degree and is in initial phase. For a long term effect and deeper effect a totality based remedy shall be taken by consulting a registered homeopathic practitioner, such a remedy helps stimulation of pancreatic cells to produce insulin and bring an overall betterment and balanced state of sugar control. These medicines can be supported by homeopathic tinctures which are at times required to bring sugar down in initial phase of treatment plan or when sugar rises beyond a certain degree. Homeopathic medicines need to be supported by correct diet management and lifestyle change which will help whatever therapy is adopted in Diabetes patients.
DIABETES MELLITUS MEDICINES3
 Acetic Acid
Acetic Acid
Large quantities of pale urine. Diabetes, with great thirst and debility. Profuse urination and sweat. Indicated in pale, lean persons with lax flabby muscles.
 Conium Maculatum
Conium Maculatum
Much difficulty in voiding. It flows and stops again. Interrupted discharge. Dribbling in old men. Increased viscidity of urinary secretion and sometimes the perspiration is augmented. The urine is said to be more abundantly secreted, to smart a little when voided.
 Gymnema Sylvestre [from Clark]
Gymnema Sylvestre [from Clark]
‘Sugar-killer’-excellent medicine for diabetes mellitus. bites. Profuse urination loaded with sugar. After passage of wine patient exclaims, ‘this passing of urine in large quantities has made me very weak’. Urine :Colour white; Quantity copious; Specific gravity high.
Insulin
Besides the use of insulin in the treatment of diabetes, restoring the lost ability to oxidise carbohydrate and again storing glycogen in liver, some use of it homoeopathically has been made by Doctor Baker. In the gouty, transitory glycosuria when skin manifestations.
 Natrium Sulphuricum
Natrium Sulphuricum
It excites the secretions of the intestines and stimulates the activity of the intestinal glands, liver and pancreas.Excessive secretion.Diabetes.
 Phosphoric Acid
Phosphoric Acid
Polyuria and dry mouth and throat give leading correspondences for its use in diabetes. The urine may be passed clear but turns milky at once and is very offensive.
 Syzygium Jambolanum
Syzygium Jambolanum
A most useful remedy in diabetes mellitus. No other remedy causes in so marked degree the diminution and disappearance of sugar in the urine. Great thirst, weakness, emaciation. Very large amount of urine, specific gravity high. Diabetes ulceration. The seeds powdered 10 grains, 3 times a day, also the tincture.
 Terebinthinea Oleum
Terebinthinea Oleum
Inflammation of the kidneys and urinary tract, with hemorrhages and strangury.Nephritis.Bright’s disease. Cystitis. Urethritis.Weakness.
REFERENCES
- Ralston S.H., Penman I.D., Strachan M.W.J., Hobson R.P. Davidson’s, Principles and Practice of Medicine. 23rdrev.ed. Edinburgh; Churchill Livingstone/Elsevier; 2018. 1417p.
- Kasper D.L., Fauci A.S., Hauser S.L., LongoD.L.,Jameson J.L., Loscalzo J. Harrison’s Manual of Medicine. 19thRev. Ed. United States: McGraw Hill; 2016,1222p.
- Boericke W. New Manual of Homœopathic Materia Medica and Repertory. 9th Reprinted Edition. New Delhi: B Jain Publishers (P) Ltd; 2005.